
Removal of Impacted Cerumen
- Home
- CPT Assistant Articles
- Removal of Impacted Cerumen
Removal of Impacted Cerumen
In the Current Procedural Terminology (CPT®) 2016 code
set, code 69209 was added to the Auditory System subsection to report the removal of impacted cerumen (earwax)
using irrigation or lavage. Impacted cerumen was defined
in CPT Assistant October 2013, page 14, as having any of
the following:
Visual considerations
Cerumen impairs exam of clinically significant portions of the external auditory canal, tympanic membrane, or middle ear condition.
Inflammatory considerations
Associated with foul odor, infection, or dermatitis.
Qualitative considerations
Extremely hard, dry, irritative cerumen causing symptoms such as pain, itching, hearing loss, etc
Quantitative considerations
Obstructive, copious cerumen that cannot be removed without magnification and multiple instrumentations requiring physician skills.
Table 1. Impacted Cerumen Removal Comparison
| Code 69209 | Code 69210 |
|---|---|
Uses irrigation or lavage |
Uses instrumentation (eg,
curettes, hooks, forceps, suction) |
May be performed by trained
office personnel under the
supervision of the physician
or other qualified health care
professional |
Requires significant physician
or other qualified health care
professional work |
Cannot be reported with code
69210 on the same day for the
same ear |
Cannot be reported with code
69209 on the same day for the
same ear |
Report the appropriate E/M code
if cerumen is not impacted |
Report the appropriate E/M code
if cerumen is not impacted |
For a bilateral procedure, append
modifier 50 |
For a bilateral procedure, append
modifier 50 |
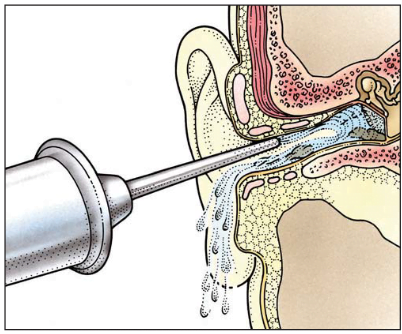
Code 69209 is reported when irrigation and/or lavage is used to remove impacted cerumen. This method uses a continuous flow of liquid (eg, saline, water) to loosen impacted cerumen and flush it out with or without the use of a cerumen softening agent. (See Figure 1.) Although direct physician work is not required, the removal of cerumen by irrigation or lavage usually takes longer to perform and may require additional staff time and equipment.
Code 69210 is reported when an instrumented approach is used for cerumen removal. The procedure must be performed by a physician or other qualified health care professional using instrumentation such as curettes, hooks, forceps, and suction to remove the impacted earwax. Only one code (69209 or 69210) may be reported for the primary service provided on the same day on the same ear. Modifier 50, Bilateral Procedure, should be appended if either one of the cerumen removal procedures is performed on both ears.
Figure 1. Irrigating Water Into Ear With Syringe (Code 69209)
Coding Tip
Codes 69209 and 69210 should not be reported together when both services are provided on the same day on the same ear.
The appropriate evaluation and management (E/M) code based upon category and site of service (eg, office or other outpatient, hospital care, nursing facility services) should be reported when nonimpacted cerumen is removed.
An E/M code may be reported if there is a separate and distinct service performed at the same session.